Ann Ostrovsky, MD
Chief of Ophthalmology, Bellevue Hospital
Acting Chief of Ophthalmology, Cumberland Clinic
Director of Keratoconus Program, NYU Langone
Co-Founder T21 Program, NYU Langone
60% of children with Down syndrome have ophthalmic conditions that need to be identified and treated in a timely manner in order to prevent long-term visual disability. Optical rehabilitation must be considered especially important in people with Down syndrome to ensure physical and mental well-being and optimize self-dependence. The majority of typical children are born far-sighted, but most will not require glasses long term as their prescriptions commonly decrease to zero, as their eyes grow. Children with Down syndrome start out far-sighted as typical children do, but in a large number, the prescriptions fail to decrease over time and 80% will need to continue to wear glasses into adulthood. Many children with Down syndrome also have high levels of astigmatism (another type of refractive error that causes objects to appear elongated) that needs to be corrected by their spectacle prescription. If the eye has a refractive error and this error is not “neutralized” with the correct glasses prescription, the child’s vision may not develop to the best of its potential. The neuronal pathways for visual development are hard-wired by around the age of 8 and so it is important to correct refractive errors for children before this critical age.
Other common eye problems in children with Down syndrome include decreased color sensitivity and difficulty with focusing on objects close up. This could actually necessitate the need for bifocal glasses in some children to optimize visual acuity at distance and near. When buying glasses, it is important to make sure your optician orders shatter-proof lenses made out of polycarbonate material. Also, because many children have a flat nasal bridge, traditional glasses frames may not fit properly. There are several companies, which manufacture special glasses frames for people with flat nasal bridges. It is important to work with opticians who have experience fitting glasses for people with flat nasal bridges. It is not always easy to convince children to wear their glasses. Some tricks to improve compliance with glasses wear include starting with wear for just a few minutes per day and then gradually increasing wearing time. Keeping kids’ hands busy with books, toys, or songs can also help with increasing cooperation with wearing glasses.
Children with Down syndrome are prone to several other eye conditions that if discovered early, can be treated to prevent problems down the road. Strabismus, or misalignment of the eyes, is one such condition. If both eyes are perfectly aligned, the images sent to the brain from each eye are identical and the brain is able to fuse those images and “process” the information. If one eye is looking in a slightly different direction than the other, the two images sent to the brain do not fuse and the brain interprets the information as double-vision. To protect itself from the double-vision, the brain suppresses the perception of images from one of the eyes. The eye from which the image is suppressed, may then develop poor vision, unless the misalignment is corrected. Eye doctors can correct this misalignment by giving the patient glasses or sometimes performing surgery to “straighten” the eyes.
Some kids with strabismus try to “align” the disparate images coming from both eyes by tilting their heads. This is another sign that we look for as a hint that there may be a misalignment between the two eyes.



Lueder GT, Arthur B, Garibaldi D, Kodsi S, Kushner B, Saunders R. Head tilt-dependent esotropia associated with trisomy 21. Ophthalmology . 2004 Mar; 111(3): 569-9.
Another eye condition that can present in children is called nystagmus, or irregular, shaking movements of the eyes. Sometimes the child is not symptomatic from this condition if it is mild, but in severe cases may cause decreased vision. If the condition causes problems, eye doctors can intervene through medical or surgical means.
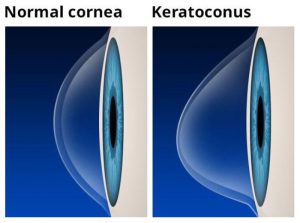
There is an increased tendency for eye rubbing in children with Down syndrome. This is a worrisome behavior as it can act as an environmental trigger for a genetic predisposition for a condition called keratoconus. Studies have shown that corneas of children with Down syndrome are thinner and weaker than those of the typical population. This underlying weakness in the structure of the cornea – the front window of the eye, can be further weakened by the mechanical action of rubbing the eyes. Over time, the normally spherical cornea can become conical in shape. This in turn results in progressive worsening of vision and even blindness. There are many interventions currently available to stop the progression and reverse vision loss caused by keratoconus. A high index of suspicion, special diagnostic testing as well as an exam by a highly specialized ophthalmologist is needed to identify this condition in its early stages. Treating any underlying allergies and discouraging eye rubbing is also very important in preventing progression of this condition.
Several other serious, but rare eye conditions should also be evaluated for during an eye examination in children include cataracts, glaucoma, congenital nasolacrimal duct obstruction, and blepharitis. It is important for all children to have routine follow-up with an eye care professional, preferably one that is familiar with the unique problems that can affect patients with Down syndrome. The American Academy of Pediatrics recommends that children with Down syndrome have their initial eye exam with a pediatric Ophthalmologist by 6 months of age, they also recommend yearly exams from 1-5 years of age, every 2 years from 5-13 years of age and every 3 years between 13-21 years of age. If the child is diagnosed with an eye condition, the visits will likely be more frequent.